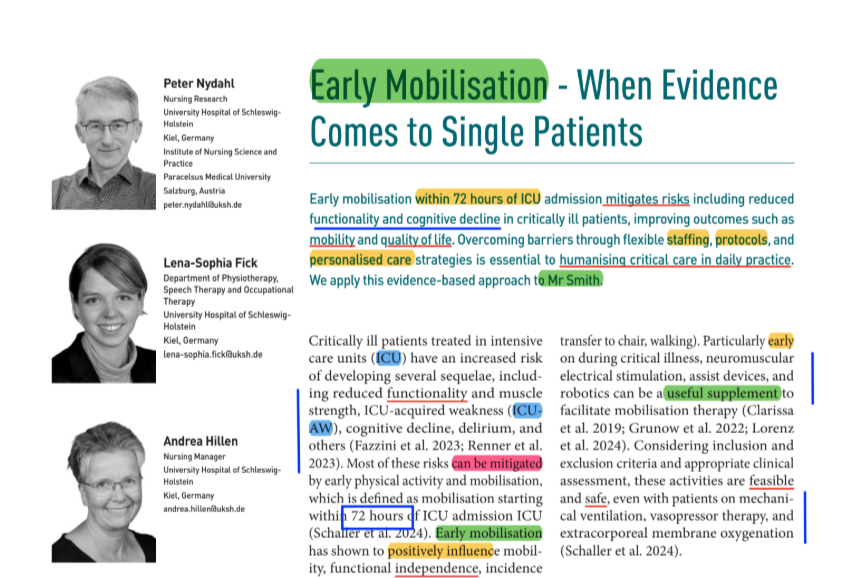
1. A JR is an academic session where we go through some articles previously codified/labeled, for 75-90 min.
2. The articles are selected during the session based on the participants interests and backgrounds.
3. Its purpose is to understand and discuss relevant content elements applying systematized note-taking methodologies.
4. We generate discussion and recall pivotal concepts about different topics, all pertinent to our clinical practice.
5. We write down the key points of every session and publish them on our website.
6. In the following session we briefly recall the key-points from the previous JR, applying the 'reinforcing technique’.
7. Check out our calendar and see you in the DISCORD server.
2024 HEALIO - Eliminating these 14 risk factors may prevent nearly half of dementia cases (AAIC).pdf
Codified by ABFL
Glossary: 🧠 = brain; AAIC = Alzheimer's Association International Conference; AGA, FPG = fasting plasma glucose (alteración de glucemia en ayunas); DEM = dementia; DIA = diabetes; Per cin = waist circumference (perímetro de cintura); RECS = recommendations; srMA = systematic review and metaanalisis.
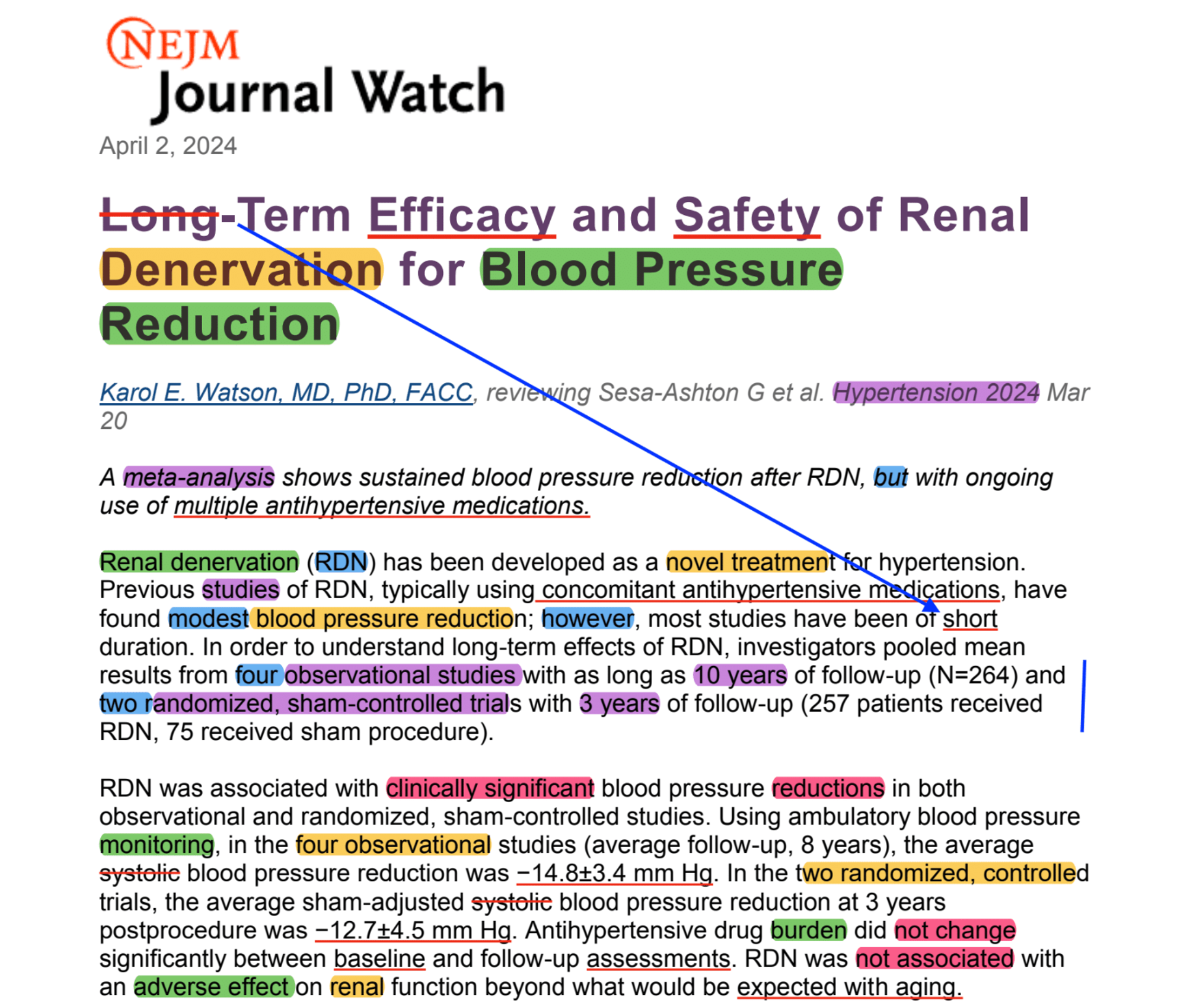
1. 14 rf, the new ones are underlined - 1/4 DEM in red:
a. ↑ 7
- pollution
- diabetes
- -ol
- -chol
- HTA
- Obesity
- Smoking
➩ HOSPdia -ol-chol
b. ↓6 - 1/3 DEM in green
- depression
- hearing
- education
- physical inactivity
- Social interaction
- vision
➩ dep-vi-so-h = “divisó”
c. =1
- head
2. 57M = DEM by 2019 ➩ expected: 153M = DEM by 2050
3. 13 RECS by Lancet comission for individuals + governments
4. Triangulation framework was used in 2020 (w_12 rf) ➩ based on srMA: all except vision loss (RR =
1.5) + LDL-chol (RR = 1.3)
- Highest: depression (RR = 2.2)
- Lowest: air pollution (RR = 1.1)
5. Implications: physicians + family physicians
6. 13 RECS ➩ the highlights:
- midlife cognitively stimulating activities (GMC)
- awareness of -ol overconsumption (AAQC)
- ↓ air pollution exposure (AMA) ➩ quantification matters (GMC)
7. Relevant association:
- Hearing ↓ ➩ social isolation ➩ -ol ➩ depression (AMA)
- ↓ physical activity ➩ iiu LDL ➩ obesity
- SM = ↑ TG + HTA + per cin + ↓ HDL + AGA or DIA (GLU>100)
⏳ TIME MANAGEMENT
01:15:53
Round: 4 10:12:50
Round: 3 58:16:30 JR
Round: 2 04:13:33 Continue
Round: 1 03:11:51 Past JR
Thursday, January 9 , 2025 at 23h30 BE ABFL, AMA, AHO, MAAT, DFM, GMC, HIBN, AAQC
⏳ TIME MANAGEMENT
01:28:34
Round: 4 01:08:07 Comment
Round: 3 21:40:72 Wrap-up
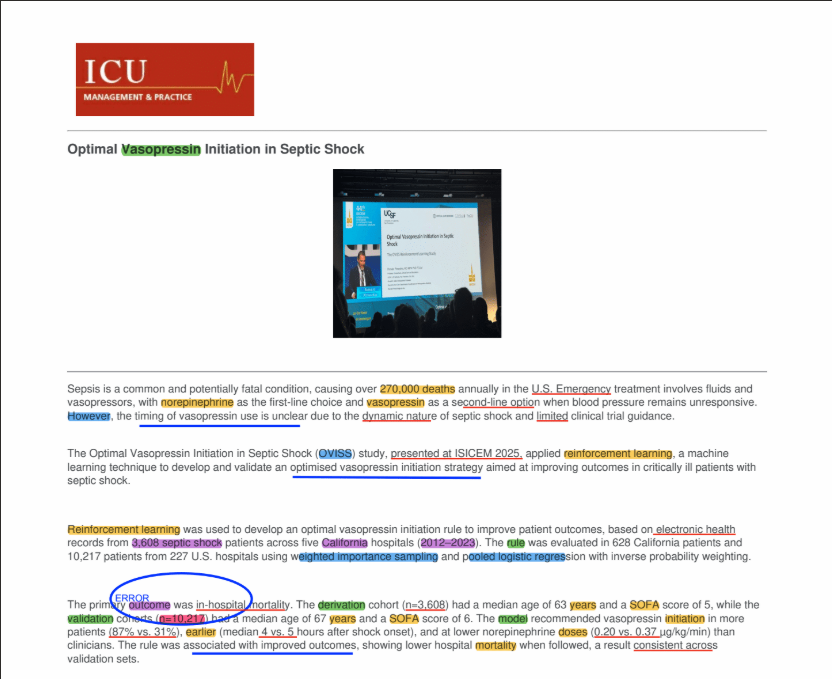
Round: 2 54:23:69 ART ➩ vasopressin
Round: 1 11:22:11 Past JR + issues
Codified by RICH
Glossary: 🫁 = lungs; 🫀 = heart; 🩸 = coagulation; MM = mortality; NE = norepinephrine; SS = Survival; SSø = septic shock; VP = vasopressin.
1. Definitions of SSØ ➩ Evans 2021 (SSC), Singer 2016 (SEPSIS-3), SSC 2012 (Dellinger)
- ↓ flow (persistent)
- ↓ pressure
- ↑ inflammation
- LIFE-THREATENING
2. SSø ➩ does NOT respond to fluids… = despite adequate volume resuscitation.
3. SSø ➩ ↑ MB + MM ➩ in ICU
4. NE (other cathecolamines) ➩ DISADVANTAGES = 🫀 + 🫁 + 🩸 + immune + METABOLISM
5. Evans 2021 ➩ SSC ➩ POTENTIAL cut-off 0.25-0.5 ug/Kg/min to add VP (despite uncertainties on
TIMING)
6. 3 retrospective OBS: (Sacha 2018, 2021 + Bauer 2022)
- PREDICTORS of VP response➩ ph + lactate
* pH ↓ = bad condition ➩ bad OC when 0,1U ↓ in pH < 7.4
* ↓ Lactate 🟰 worse 🆚 best 🟰 5.4 🆚 4, p<0.001
- H+_MM ➩ NE dose + lactate
* ↓ NE 🟰10ug/min ✔ 🆚 up to 60ug/min ✖ ➩ ↑ ↑ iH+_MM w_10ug/min (additional to 60ug/min)
▶ 21%
* ↓ Lactate 🟰 2.3 mmol/L ✔ ➩ ↑ every 1mmol/L ✖ ➩ ↑ ↑ iH+_MM w_each_1mmol/L ▶ 18%
7. VASOPRESSIN RESPONSE = while MAP ≥65mmHg + ↓ NE d_6h ➩ under VP
8. Perspectives + hopes + realities ➩ explanation.
Monday, January 6 , 2025 at 23h30 BE ABFL, AMA, AHO, MAAT, DFM, GMC, HIBN, AAQC
2018 CID - Renal Dosing of Antibiotics Are We Jumping the Gun (Crass) [r].pdf
Codified by ABFL
Glossary:
🫁 = PNA = bacterial pneumonia;
ABSSI = acute bacterial skin and skin structure infections;
AKI = acute kidney injury;
CID = clinical infectious diseases;
CrCL = creatinine clearance;
cUTI = complicated urinary tract infection;
GFR = glomerular filtration rate;
ICD = International Classification of Diseases;
cIAI = complicated intraabdominal infections
REC = record
1. 𝙄𝙌𝘾 BS ➩ Y, J, C ➖ T ➕ N ➕ t ➖ P I C O:
2. 𝙄𝙌𝘾 BS 🟰 2018, CID, USA (Michigan) ➖ retro_REC ➕ 18500 ➕ 2006-2018 ➖ P I C O:
- P: adults w_ID (cUTI + cIAI + PNA + ABSSI)
- I: AKI OR moderate impairment
- C: NA
- O: transient OR persistent
3. METHODS.
- DEF ➠ cUTI = ≥56yo
- 3 equations were used: Cockcroft-Gault (CrCL) + MDRD (eGFR) + CKD-EPI (eGFR)
- IN ➠ ICD 9th and 10th (admitting, primary or present) + only 1st encounter
- EX ➠ >1 infection type + CKD ≥S4 + incomplete or inaccurate REC + Scr <3
4. RESULTS
- Scr 0.88 in all + ↑ “♾ 0.94 + ABSSSI 0.84” than “🫁 0.81+ 🫃🏽0.8”
- AKI at admission = 17.5%, most common in 🫁
- less common = ABSSSI 9.7%
- AKI resolves in 57,2% ➩ in 48h
- Moderate renal impairment ➩ 43-46% had ↗ ➩ GFR >50 ➩ in 48h
⏳ TIME MANAGEMENT
01:12:25
Round: 3 25:52:42 Wrap-up
Round: 2 35:47:33 Continue last JR
Round: 1 10:45:96 Past JR
Thursday, January 16, 2025 at 23h30 BE MAAT, AHO, DFM, GMC, JCAU, RICH, HIBN, AAQC
2018 CID - Renal Dosing of Antibiotics Are We Jumping the Gun (Crass) [r].pdf
Codified by ABFL
Glossary: [IS] = Israel; ♾ = kidneys = renal; 🫁 = lungs; ATB = antibiotic; CART = classification and regression tree analysis; ID = infectious disease; ID = infectious diseases; INF = infective; MOO = microorganism; TTO = treatment.
1. CRITICAL PERIOD ➩ primary driver of ID = early ATB TTO
2. Adequate ➩ doses = ATB in vitro → target pathogens = ATB in vivo (pharmacodynamics)
3. Early ➩ empirical TTO period… WHEN INF moo + susceptibility = unknown.
4. DATA:
- Retro_cohort (SSø) ➩ 14 ICU + 10 H+ ➩ 1h delay = ↓SS (7.6%)
- MA (S) ➩ ✖ 48h = ↑MM (1.6OR) ➩ NNT = 10
- SingleCen_OBS (BSI) ➩ [IS] + ✖ = ↑ MM (1.6 OR)
* intra 🫃🏽= ↑ MM (3.8OR)
* skin = ↑ MM (3.1OR)
- Retros_cohort (comm_acq_BSI) ➩ ✔ 48h = ↓MM (0.54 OR)
- Pros_S (BSI_Enterococcus) ➩ ✔ 48h = ↓MM (0.21 OR)
- Retros_singC (BSI_Enterococcus) ➩ ✖ outside CART (48.1h) = ↑MM (3x)
- OBS_USA (BSI_S. aureus) ➩ ✔ CART (44.75h) = ↓ MM
5. ✔ pharmacodynamic = dosis + administration (although ok in vitro ↔ in vivo activity)
6. 48h = CRITICAL IMPORTANCE ➩ ↓ doses in ♾ impairment = poor
OC (IF impairment does not persist)
⏳ TIME MANAGEMENT
01:12:56
Round: 5 06:12:25
Round: 4 08:57:76 Wrap-up
Round: 3 44:03:93 Continue w_JC
Round: 2 07:49:54 ART selection
Round: 1 05:52:77 Past JR
Monday, January 13 , 2025 at 23h30 BE ABFL, AMA, AHO, MAAT, DFM, GMC, HIBN, AAQC
2024 NEJMjw - PREVENT A New Cardiovascular Risk Calculator (JAMA).pdf
Codified by ABFL
Glossary:
🫀 = heart; ACC/AHA = American College of Cardiology/American Heart Association; CHOL mm = Cholesterol management; JAMAim = JAMA internal medicine; MI = myocardial infarction; S† = stroke.
1. New CV risk calculator ➩ PREVENT
2. PREVENT is from AHA 🆚 past one from AHA & ACC 2013
3. Comparison:
- Much larger + more contemporary (derived from databases)
- 5 new input variables:
* 2 mandatory: BMI + eGFR
* 3 optionals: HbA1c + urinary albumin-creatinine ratio + zip code (social deprivation)
- No RACE
- Adds ‘CARDIOVASCULAR DISEASE' = heart failure + ASCVD (past one ONLY ASCVD)
- All published in CIRCULATION 2024
4. Comparison ↔ current PREVENT 🆚 older calculator
- 2 studies ➩ 2024 JAMAim, JAMA, US, wo_MI or S† ➩ PREVENT (4-5%) 🆚 older (8-9%)
- Same studies = considered ↓ adults for PRIMARY preventive STATIN
5. Decision making in primary care?
- 2024 Editorial ➩ continue w_2018 ACC/AHA GL on CHOL mm
- Consider the 7.5% threshold ➕ pxs preferences
- Next version of the GL will address the LOWER RISK ESTIMATES (PREVENT)
⏳ TIME MANAGEMENT
16:56:41
Round: 4 00:00:95
Round: 3 00:46:06 Comments
Round: 2 09:17:87 Wrap-up
Round: 1 06:51:52 Selection + reading
Codified by ABFL
1. AI models demonstrated:
- Expert-like reasoning performance
- Human-like cognitive biases
2. LLM = GPT-4 + Gemini-1.0-Pro
3. Contextual factors are not considered by AI ➩ can't easily be captured in written clinical vignettes
4. Study ➩ 50 physicians ➩ randomized:
- Group A. USE OF Standard DX tools
- Groups B. USE OF Standard DX tools ➕ GPT-4
- Results: DID NOT enhance dx performance (…+GPT-4)
- Interpretation: LLM does not outperform humans BUT humans (physicians) need more training to
use LLM.
Monday, January 27, 2025 at 23h30 BE AMA, AHO, MAAT, GMC, HIBN, AAQC
⏳ TIME MANAGEMENT
01:06:04
Round: 10 00:11:29 Final comments
Round: 9 05:10:62 Wrap-up
Round: 8 04:42:22 Analysis
Round: 7 04:10:13 ART 2
Round: 6 00:26:19 Final comments
Round: 5 18:30:33 Wrap-up
Round: 4 14:53:35 Analysis
Round: 3 05:38:23 Hyponatremia
Round: 2 04:50:40 ART selection
Round: 1 07:31:32 Past JR (Andrea)
2024 NEJMjw - Treating Hyponatremia, Pick Up the Pace (JAMA).pdf
Codified by ABFL
Glossary:
♾ = kidneys = renal; 🫀 = heart; ACC = American College of Cardiology;
AHA = American Heart Association; Coh = cohort; im = internal medicine;
Mass = MAssachusetts; ODS = osmotic demyelination syndrome
1. 𝙄𝙌𝘾 BS ➩ Y, J, C ➖ T ➕ N ➕ t ➖ P I C O:
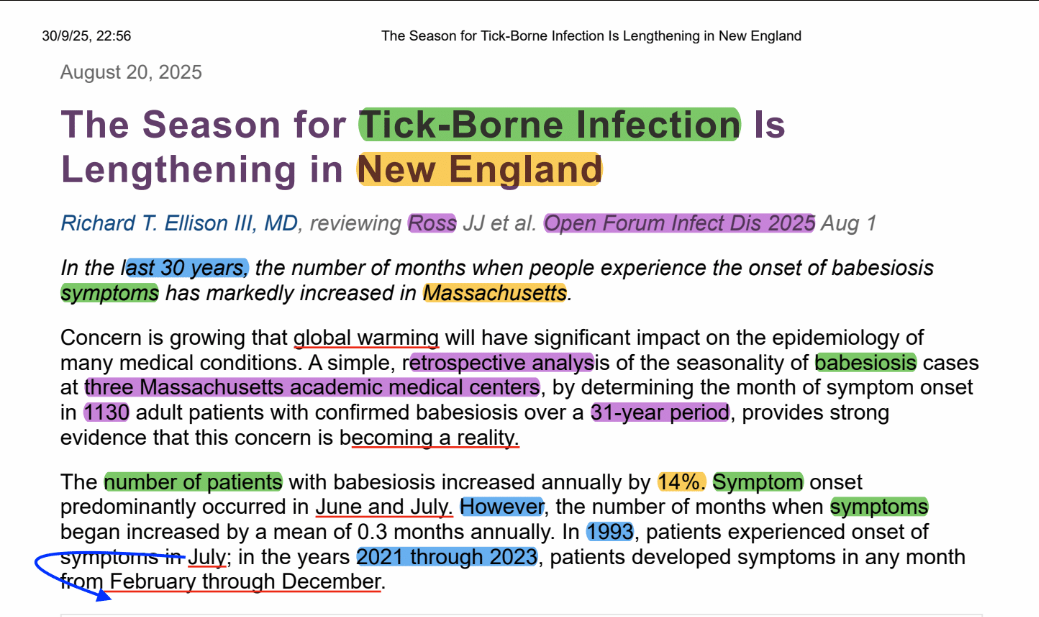
2. Study 1. 🟰 2023, NEJM evidence, USA (2H+ in Mass) ➖ retros ➕ 3000 ➕ 25y ➖ P I C O:
- P: adults, severe hyponatremia (Na < 120)
- I: slow 🆚 fast CORRECTION (<6mEq / 24h 🆚 >10mEq / 24h)
- C: NA
- O: MM ➩ Result: ↑ MM in SLOW correction
- RESULTS: slow ↔ ↑ H+_MM➕ fast ↔ shorter H+_stay & (somewhat) ↓ MM ➩ ODS = 0.2% (7 pxs, overall incidence)
3. Study 2. 🟰 2024, JAMA im, NA ➖ MA ➕ 16 coh (12k)➕ ? ➖ P I C O:
- P: adults, severe hyponatremia
- I: cases of ↓ Na (Na <120 OR Na < 125 w_sev_SYMP)
- C: NA
- O: H+_MM & MM30 ➩ Result: ↓ in FAST
- RESULTS: Thesholds varied ➕ slow 🆚 fast CORRECTION (6 🆚 10 in 24h) ➩ ODS ≤0.5% (overall incidence)
4. RATIONALE
- All the studies were OBSERVATIONAL ➩ risk of unmeasured confounders
- Might NOT apply to MOST-SEVERE hyponatremia (although there is robust evidence of a fast
correction)
- Several studies suggest that we should be correcting hyponatremia more rapidly.
2024 NEJMjw - PREVENT A New Cardiovascular Risk Calculator (JAMA).pdf
Codified by ABFL
1. New CV risk calculator ➩ PREVENT
2. PREVENT is from AHA 🆚 past one from AHA & ACC 2013
3. Comparison:
- Much larger + more contemporary (derived from databases)
- 5 new input variables:
* 2 mandatory: BMI + eGFR
* 3 optionals: HbA1c + urinary albumin-creatinine ratio + zip code (social deprivation)
- No RACE
- Adds ‘CARDIOVASCULAR DISEASE' = heart failure + ASCVD (past one ONLY ASCVD)
- All published in CIRCULATION 2024
Thursday, January 23, 2025 at 23h30 BE ABFL, AMA, AHO, MAAT, HIBN, AAQC
Codified by ABFL
Glossary: AI = artificial intelligence; LLM = large language models; RA = Rheumathoid arthritis.
1. AI models demonstrated:
- Expert-like reasoning performance
- Human-like cognitive biases
2. LLM = GPT-4 + Gemini-1.0-Pro
3. Contextual factors are not considered by AI ➩ can't easily be captured in written clinical vignettes
4. Study ➩ 50 physicians ➩ randomized:
- Group A. USE OF Standard DX tools
- Groups B. USE OF Standard DX tools ➕ GPT-4
- Results: DID NOT enhance dx performance (…+GPT-4)
- Interpretation: LLM does not outperform humans BUT humans (physicians) need more training to use LLM.
5. 3 types of bias of AI in this study:
- Framing effect. Decisions influenced by how information is presented ➩ recommended surgery
EXPRESSED as SS (34% by 5y) instead of high MM (66% by 5y)
- Primacy effect. Tendency to better remember the first piece of information they encounter than
the information they receive later on. ➩ PE as top 3 DX (hemoptysis mentioned first) 🆚 PE as
top 3 DX but not iteratively (hemoptysis NOT mentioned first OR less emphasized).
- Hindsight effect. Phenomenon that allows to convince oneself after an event that they accurately
predicted it before it happened. ➩ soft tissue inflammation ➩ one version PX died 🆚 other
version recovered, although GPT-4 said “irrespective of the outcome”… appropriate care has
provided to the first case.
6. AI wo_critical lens could exacerbate decision-making errors.
7. Talk to AI, and make open questions:
- Does this patient have rheumatoid arthritis? ✖ 🆚 Can you provide evidence against a DX of RA?
✔
- What is the likely diagnosis? ✖ 🆚 What are likely diagnoses that could explain these symptoms?
✔
2025 HBR - The Surprising Power of Team Rituals (Zakhour) [r].pdf
Codified by HIBN
1. We could apply the team rituals in our current workplaces
2. Work rituals = collective activities that members of a team engage in regularly and to which they
attribute meaning.
3. 𝙄𝙌𝘾 BS ➩ Y, J, C ➖ T ➕ N ➕ t ➖ P I C O:
4. 2025, Cosmic Centaurs, USA ➖ survey ➕ 929 individuals (60 countries) – field study (UAE, SA, L)➕ 3y ➖ P I C O:
- P: teams different enterprises (survey) + from advertising agency (field study)
- I: questions + high use of rituals
- C: NA + low use of rituals
- O: purpose + phychological safety + interpersonal knowledge + job satisfaction ➩ work
experiences + barriers to implementation + design and complying.
5. To design ➕ implement a successful set of rituals ➩ 5 measures:
- Leading w_faith
- Imbuing rituals w_meaning
- Being religious about participation
- Keeping the faith but adapting the practice
- Spreading the word6. Effective communication (AMA) – consistent application (HIBN) – start the
habit (AAQC).
⏳ TIME MANAGEMENT
01:33:32
Round: 7 03:20:03 Comments
Round: 6 14:59:69 Wrap-up
Round: 5 29:54:11 ART 2
Round: 4 10:41:46 Wrap-up
Round: 3 23:06:63 Continue past JR
Round: 2 03:19:20 Comments
Round: 1 08:11:14 Past JR
Thursday, January 30, 2025 at 23h30 BE ABFL, AMA, AHO, GMC, JCAU, MACR, HIBN, AAQC
⏳ TIME MANAGEMENT
01:14:09
Round: 8 00:42:44 Comments
Round: 7 17:29:60 Wrap-up
Round: 6 13:57:03 ART 2
Round: 5 06:00:31 ART selection
Round: 4 00:37:48 Comments
Round: 3 16:22:15 ART 1
Round: 2 12:12:32 2nd Past JR by AHO
Round: 1 06:47:86 Past JR by AMA
2025 NEJMjw - Are SGLT-2 Inhibitors Safe and Effective in H+ pxs (DC).pdf
Codified by MAAT
Glossary:
🫀 = heart; ♾ = kidneys = renal; AKI = acute kidney injury;
DKA = diabetic ketoacidosis; DM = diabetes mellitus; INF = infection.
1. 𝙄𝙌𝘾 BS ➩ Y, J, C ➖ T ➕ N ➕ t ➖ P I C O:
2. 𝙄𝙌𝘾 BS 🟰 2024, DC, NA ➖ MA ➕ 20k ➕ ❓ ➖ P I C O:
- P: DM pxs + HF (hospitalized)
- I: SGLT-2 ⊖ ✔
- C: SGLT-2 ⊖ ✖
- O: pOC = DKA | sOCs = readmission + MM + AKI
3. EVIDENCE:
- SGLT-2 ⊖ is IMP ➩ DM + ♾ disease + 🫀 failure
- Little is know about risks + benefits
- Chief concern = DKA (results from INF + ↓ oral intake)
- Euglycemic ketoacidosis 🆚 hypergycemic ➩ former could be missed
4. RESULTS
- 30% were DM
- DKA = ↑ SGLT-2 receivers (non-significant) = 0.21 🆚 0.14 per 100 person-years
- Readmission ↓ (significantly)
- MM ↓ in 🫀failure pxs
- ♾ injury ↓ incidence
- OBS studies (20) DID NOT show ↑r_DKA w_SGLT-2 ⊖
5. RATIONALE
- Caution w_INTERPRETATION (nonsignificant)
- Results underpowered ❓
- Risk underestimated due to IN outPXS follow-up
- Supports SGLT-2 ⊖ use in H+ w_🫀 failure
2025 HBR - The Surprising Power of Team Rituals (Zakhour) [r].pdf
Codified by HIBN
Glossary:
m = months
1. Being religious about participation.
- Easy 🆚 Hard ➩ selecting + designing 🆚 disciplined (communicating + organizing + engaging)
- RITUAL is a CORE ASPECT (not optional, not extracurricular)
- FOR teams NEW TO RITUALS ➩ no all in one, but ONE AT A TIME (sequentially) ➖ ritual owner
= develop: relevant communication + agendas + templates (it should be CHANGED or ROTATED
regularly)
- Field study ➩ 3m ➩ at departure (turnovers + strategy shifts) theaters of stopping the rituals ➩ 6m
later, the survey showed they kept the rituals (82% high levels of observance)
2. Keeping the faith but adapting the practice..
- A good operating system is one that adapts over time ➩ according to CONTEXT
- 6-12m ➩ rituals should be reviewed (purpose + relevancy)
- Cancel the RITUALS that do not serve you (add new ones ➩ needs + preferences + cultural
context)
- Andrea (AMA): Cultural context ➩ punctuality as a good habit despite her cultural context
- Hans (HIBN): What the team prefers, needs and how their context influences them. Alcohol
example
- Frequencies should also ve REVISITED.
3. Spreading the word.
- One committed leader IS essential
- Preach the RITUAL value to the broader organization once it bears FRUIT
- The help teaching + sharing + helping
- Certainty + connection + engagement are the RESULTS
Monday, February 10, 2025 at 23h30 BE AMA, AHO, BAR, DFM, MACR, RCH, HIBN, AAQC
2025 HBR - The Surprising Power of Team Rituals (Zakhour) [r].pdf
Codified by HIBN
1. We could apply the team rituals in our current workplaces
2. Work rituals = collective activities that members of a team engage in regularly and to which they attribute meaning.
3. 𝙄𝙌𝘾 BS ➩ Y, J, C ➖ T ➕ N ➕ t ➖ P I C O:
4. 2025, Cosmic Centaurs, USA ➖ survey ➕ 929 individuals (60 countries) – field study (UAE, SA, L)➕ 3y ➖ P I C O:
- P: teams different enterprises (survey) + from advertising agency (field study)
- I: questions + high use of rituals
- C: NA + low use of rituals
- O: purpose + phychological safety + interpersonal knowledge + job satisfaction ➩ work experiences + barriers to implementation + design and complying.
5. To design ➕ implement a successful set of rituals ➩ 5 measures:
- Leading w_faith
- Imbuing rituals w_meaning
- Being religious about participation
- Keeping the faith but adapting the practice
- Spreading the word
6. Effective communication (AMA) – consistent application (HIBN) – start the habit (AAQC).
7. LEADING w_faith
- Commitment is ESSENTIAL to start rituals.
- In the field study, skepticism was high… then everyone started to participate (first the CEO).
- Engagement and faith is important among the team members ➩ one member co-created a check-
in ritual.
8. IMBUING RITUALS w_meaning
- Not a religious connotation but meaning
- The purpose MUST be aligned w_specific goals (WHAT) + organizational purpose (WHY)
- 5 GOALS IN THE study: 1) strategy and planning, 2) performance management, 3) improving operations, 4) learning, and 5) team engagement and relationship-building
- One member co-created a monthly ritual and they met to follow the PROCESS as a team (rather than PROGRESS)
- Earlier interventions are useful
- RETROSPECTIVE ➩ had certain points: purpose + facilitated discussions of reflections &
suggestions + mutual commitment towards action steps.
– No finger-pointing and defensiveness.
- No work topics were discussed during these “TEAM TIME”
- QUESTIONS to use: “What part of your childhood would you change if you could?” and “How do
you like to receive negative feedback?”
9. Being religious about participation.
- Easy 🆚 Hard ➩ selecting + designing 🆚 disciplined (communicating + organizing + engaging)
- RITUAL is a CORE ASPECT (not optional, not extracurricular)
- FOR teams NEW TO RITUALS ➩ no all in one, but ONE AT A TIME (sequentially) ➖ ritual owner
= develop: relevant communication + agendas + templates (it should be CHANGED or ROTATED
regularly)
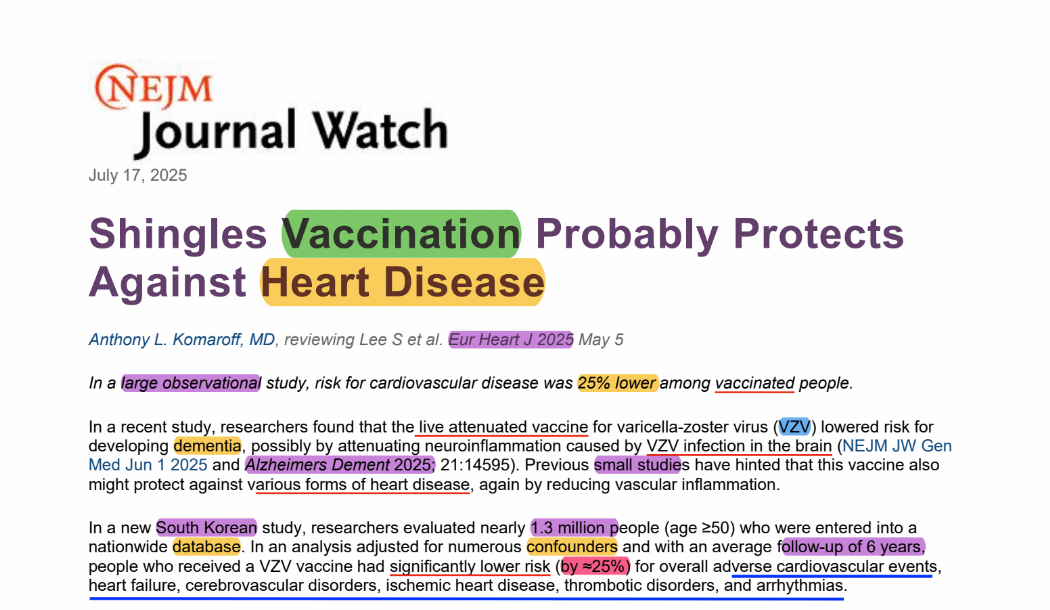
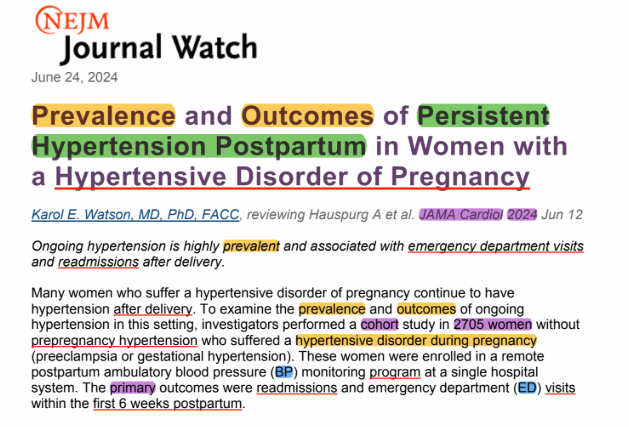
2025 NEJMjw - Is “As-Needed” Blood Pressure Medication Really Needed in inPXS (JAMA).pdf
Codified by ABFL
Glossary: BP = blood pressure; HR = hazard ratio; JAMAim = JAMA internal medicine; MI = myocardial infarction; QX = surgical; S† = stroke; TTO = treatment = medication.
1. 𝙄𝙌𝘾 BS ➩ Y, J, C ➖ T ➕ N ➕ t ➖ P I C O:
2. 𝙄𝙌𝘾 BS 🟰 2025, JAMA im, ? ➖ RETROSPECTIVE ➕ 130k ➕ ? ➖ P I C O:
- P: adults, 71yo ➩ hospitalized (Veteran affairs)
- I: as-needed BP TTO
- C: NA (“nonrecipients”)
- O: AKI ➖ composite: MI ➕ S† ➕ MM
3. EVIDENCE:
- Hypertension 2024 ➩ OBS studies
- Consensus ➩ NOT to use “as-needed” BP TTO
4. METHODS.
- IN ➠ CV related admission + antiHTA TTO + SBP >140
- EX ➠ QX + ICU pxs
6. RESULTS
- 21% received as-needed BP TTO
- Propensity-score ➩ AKI excess (HR 1.2) = as-needed BP TTO ➕ 💉 as-needed BP TTO =
MORE AKI excess (HR 1.6)
- Secondary analyses ➩ as-needed BP TTO: BP drop (1.5-fold) + composite (MI + S† + MM) 🆚 non recipients
7. RATIONALE
- Do not treat a NUMBER
- DO not order as-needed BP TTO
- Do not write a BP THRESHOLD to automatically start BP TTO
8. COMMENTS
- Careful with technology automated thresholds (AMA)
⏳ TIME MANAGEMENT
01:37:51
Round: 5 01:23:30 Comment
Round: 4 32:03:26 ART 2
Round: 3 10:22:43 Comments
Round: 2 41:58:71 ART1: Continue ART2 last JR
Round: 1 12:04:22 Past JR
Monday, February 3, 2025 at 23h30 BE ABFL, AMA, AHO, MAAT, DFM, JCAU, HIBN, AAQC
⏳ TIME MANAGEMENT
01:52:33
Round: 8 00:37:70 Final comments
Round: 7 12:16:39 wrap - up
Round: 6 27:07:68 Comments
Round: 5 31:59:68 Exploration
Round: 4 01:40:88 Comments
Round: 3 30:13:56 ART 1
Round: 2 01:25:47 ART Selection
Round: 1 07:11:64 Past JR
2025 CC - Physiology and pathophysiology of mucus + mucolytic use in CrIll pxs (Roe) [r].pdf
Codified by AMA
Glossary:🫁 CA = lung cancer; CF = cystic fibrosis; COPD = chronic obstructive pulmonary disease; DYS = dysfunction; GL = guidelines; INF = infection; MV = mechanical ventilation; MV = mechanical ventilation.
1. Start by the same article next JR (see images, figures, tables) ➩ mucus dysfunction
2. Airways mucus ➩ lubricating ➕ humidifying
3. DYS (CI pxs) ➩ changes in production ➕ composition➕ physical properties ➕ inflammatory phenotype
4. MUCUS:
- Water
- Proteinas
- Lipids
- Carbohydrates
- Electrolytes
5. Function ➩ lubricant 💦 + air humidification 💨 + selective permeable barrier 𝌉 (gas exchange & nutritional absorption)
6. Main diseases w_mucus DYS:
- Asthma
- COPD
- CF
- 🫁 CA
7. ICU factors lead to CHANGES IN mucus:
- INF
- Accumulation of inflammatory cells
- 🫁 ↓ H2O
- ↓ 😷 reflexes
- ↑ O2
- MECH stress from MV
8. Survey 2020, UK ➩ 4% uses or follows GL (83% uses it as normal practice)
9. Morphological CHANGES, epitelium from 🐽 to 👛ALV:
- HIGH ➩ = ciliated
- LOW ➩ cuboidal
10. CELLS
- Secretory (submucosal) ➩ production of MUCUS ➩ 60% of gland volume (98% water, 1%
salts, 0.3% mucin glycoproteins)
- Ciliated (epithelial) ➩ movement of MUCUS
11. Mucin glycoproteins properties:
- Antimicrobial
- Immunological
- Defensive
Monday, February 24, 2025 at 23h30 BE AAGC, AG, AMA, AHO, MAAT, IC, JQB, JV, KG, LL, PACG, VV, N, HIBN, AAQC
⏳ TIME MANAGEMENT
01:17:49
Round: 4 47:56:59 Comments
Round: 3 14:13:90 ART
Round: 2 05:52:89 ART selection
Round: 1 09:46:44 Past JR
Codified by 𝙄𝙉𝘼𝘼𝙌𝘾 ᴮᴼ (ABFL)
Glossary: BSIs = bloodstream infections, INF = infection, SØ = septic shock
1. 𝙄𝙌𝘾 BS ➩ Y, J, C ➖ T ➕ N ➕ t ➖ P I C O:
2. 𝙄𝙌𝘾 BS 🟰 2025, JAC, IT ➖ retro_OBS ➕ 170 pxs (14 H+) ➕ ? ➖ P I C O:
- P: ICU pxs w_BSIs
- 🅸: antiPseudo therapy: 22% pip-taco, 43% carbap, 7% colistin, 28% newer cephalosporins
(ceftolozane/tazobactam, ceftazidime/avibactam, or cefiderocol) >48h
- 🅲: NA
- O: pOC = predictors of MM30 (definitive antimicrobial)
3. EVIDENCE:
- BSIs is common in the ICU
- Effects on OCs of the ATB TTO is lacking.
4. RESULTS
- 1/3 ➩ SØ
- 23% ➩ carbs-resistant INF
- Analysis adjusted (obs BIAS):
* ↓ MM in overall ➩ novel antiPseudo cephalosporins
* ↓ MM in SØ ➩ combination therapy ⏤ ATB❓
5. RATIONALE
- Although high rates of carbs RESISTANCE (>20%), SAME BENEFIT.
- This population (hr_pxs w_P. Areruginosa bacteremia in ICU) of pxs SHOULD be included in future
CLINICAL TRIALS (this is a retrospective observational study).
Thuesday, June 12, 2025 at 23h30 BEAMA, AHO, HIBN, AAQC